Introduction
Healthcare and benefits data doesn't live in one place. It's scattered across HRIS platforms, payroll providers, insurance carriers, benefits administrators, and EHRs — each with its own data model, authentication method, and API maturity level.
For engineering teams building HR Tech, Benefits Tech, or Insurtech products, that fragmentation has real consequences: integrations break during open enrollment, eligibility data goes stale, and onboarding a new employer takes weeks instead of hours.
The compliance layer compounds that fragmentation. Any integration touching Protected Health Information (PHI) or employee benefits data carries HIPAA obligations — and teams that don't design for compliance from the start typically discover the gaps during an audit, not before.
According to HIPAA Journal, hacking-related healthcare data breaches increased 239% between January 2018 and September 2023. Third-party vendors were linked to 37% of healthcare breaches in 2025. The integration layer is a primary attack surface — and it deserves the same engineering discipline as the core product.
This guide covers the integration challenges, security and compliance requirements, interoperability standards, architecture decisions, and maintenance practices engineering teams need to build healthcare API integrations that hold up in production.
TL;DR
- Healthcare API integration connects HRIS, payroll, carrier, and EHR systems to enable real-time eligibility, enrollment sync, and benefits data workflows
- HIPAA compliance requires OAuth 2.0 auth, TLS 1.2+ encryption, audit logging, and signed BAAs with every vendor touching PHI
- HL7 FHIR covers clinical data; EDI X12 (834, 270/271) drives carrier and benefits connectivity — your integration stack needs both
- Architecture decisions — unified API vs. point-to-point, webhook design, legacy handling — determine long-term maintenance burden more than anything else
- Proactive monitoring, version management, and dead letter queues are what separate integrations that scale from those that break under load
Key Challenges in Healthcare API Integration
Healthcare API integration is harder than most B2B integration work — not because the technology is unusually complex, but because the ecosystem has three structural problems that don't appear in other domains.
Fragmentation Across Incompatible Systems
The US healthcare IT market is fragmented. Epic holds 42.3% of the acute care EHR market as of 2024 (KLAS Research via Fierce Healthcare), meaning the remaining ~58% is split across dozens of competing vendors.
Add in the HRIS landscape — ADP, Workday, UKG, Rippling, BambooHR, Gusto, Paychex, and hundreds of regional systems — plus insurance carriers and benefits administrators, and you're looking at hundreds of systems with incompatible data models.
A connection built for one system rarely transfers to another. Field names, authentication methods, rate limits, pagination behavior, and data freshness guarantees all vary by vendor. Every new integration starts from scratch unless the team has invested in abstraction.
The Compliance Burden Is Unique to Healthcare
Every integration that touches PHI or employee benefits data triggers HIPAA obligations. The difference from other B2B data work:
- Every vendor in the data flow needs a signed Business Associate Agreement (BAA) before data flows through their systems
- Audit logs must be retained for a minimum of six years under 45 CFR 164.530(j)
- Access controls, encryption, and incident response must be documented and enforced — not just implemented
Teams that skip compliance-first design typically discover the gaps during audits — facing remediation costs, potential fines, and the work of rebuilding integrations that weren't built to spec.
Legacy Systems Aren't Going Away
A significant portion of insurance carriers and HR systems still export data via SFTP file drops and HL7 v2 batch feeds. This isn't a temporary situation — HIPAA-mandated EDI transactions (X12 834 for enrollment, 270/271 for eligibility) were built for batch exchange.
Carrier systems were designed around that paradigm, and most haven't moved away from it.
Skipping these systems isn't an option — they hold the eligibility and enrollment data that the rest of your stack depends on. Teams need to plan for:
- Modern REST API connectivity for systems that support it
- Legacy SFTP ingestion for batch file exports
- HL7 v2 and EDI parsing for carrier and insurance data flows
Security and Compliance Best Practices
Implement Strong Authentication and Authorization
OAuth 2.0 with scoped tokens is the standard for healthcare API authentication. The ONC explicitly recommends OAuth 2.0, and the SMART App Launch Framework profiles it specifically for FHIR resource access.
Why it matters beyond general security: scoped tokens limit the blast radius when credentials are compromised. A token scoped to read-only eligibility data can't be used to modify enrollment records. Key requirements from the SMART App Launch spec:
- All apps must support PKCE (Proof Key for Code Exchange)
- Access tokens should have a lifetime no greater than one hour
- All transmission occurs over TLS-secured channels only
Every API consumer — internal services, third-party vendors, partner platforms — receives only the minimum permissions required for its specific function. That minimum-permission scope only holds up if access is reviewed on a defined cadence, not just configured once at onboarding.
Enforce Encryption at Every Layer
All data in transit must use TLS 1.2 or higher. Data at rest — databases, file storage, logs containing PHI or benefits data — must use AES-256 or an equivalent standard.
"Encryption in transit only" is a common gap. Data stored downstream in log aggregators, data warehouses, or intermediate processing systems is just as exposed as data in motion. Treat every storage destination as a potential exposure point, not just the wire.
Encryption key management is the detail that often gets skipped:
- Use a dedicated Key Management Service (KMS) rather than hardcoding keys in application config
- Document and enforce key rotation schedules
- Never store encryption keys alongside the data they protect
Maintain HIPAA Compliance Throughout the Integration Lifecycle
Business Associate Agreements are non-negotiable. Under 45 CFR 164.502(e) and 164.504(e), any vendor that creates, receives, maintains, or transmits ePHI on your behalf is a business associate — including API gateway providers, cloud infrastructure, and integration middleware. A BAA must be executed before any PHI flows through their systems.
A HIPAA-compliant data handling policy for API integrations covers four areas:
- Request and store only the fields the integration actually needs — not entire records
- Define how long each data type is retained, then enforce automated deletion against that schedule
- De-identify at the integration layer when full PHI isn't required downstream
- Maintain an incident response plan that's documented, tested, and current — not a first-draft document sitting in a shared drive
When evaluating API vendors and integration partners, require independently verified compliance certifications — SOC 2 Type II, ISO 27001, and HIPAA attestation — rather than self-reported compliance claims. External audits mean the controls have actually been tested, not just described in a policy document.
Bindbee, for example, maintains SOC 2 Type II, ISO 27001, and HIPAA compliance across its integration infrastructure — the baseline any benefits or HR Tech team should require from an integration layer they depend on.
Establish Audit Trails and Conduct Regular Security Reviews
Comprehensive API audit logs are both a HIPAA requirement (45 CFR 164.312(b)) and an operational necessity. Every log entry should capture:
- Timestamp and request ID
- Source system and data type
- Operation performed and response code
- Latency and the identity of the requesting principal
Logs must be tamper-evident and retained for a minimum of six years. Structured logging (JSON format) enables automated parsing and dashboarding — essential when managing integrations across many systems simultaneously.
Security review cadence:
- Automated vulnerability scanning on every deployment
- Penetration testing periodically (at minimum annually)
- Formal compliance audits at least once per year
Reviews should cover the entire data flow from source system to consumer, not just the API endpoints themselves.
Interoperability and Data Normalization Best Practices
Adopt Recognized Healthcare Data Standards
Two standards dominate healthcare and benefits data exchange, and teams building in this space need to support both:
HL7 FHIR is the current standard for clinical data exchange. It uses RESTful API conventions and standardized resource types — Patient, Coverage, Claim, Practitioner — that allow different systems to exchange data without custom transformation logic. FHIR R4 is now mandated by CMS for Medicare Advantage, Medicaid, CHIP, and QHP issuers under the CMS Interoperability and Patient Access Final Rule (CMS-9115-F), with Patient Access API compliance enforced since July 2021.
EDI X12 remains dominant for insurance and benefits administrative workflows:
| Transaction | Purpose |
|---|---|
| X12 834 | Benefit enrollment and maintenance between sponsors and payers |
| X12 270/271 | Eligibility inquiry and response between providers/employers and payers |
FHIR is not replacing EDI for carrier connectivity anytime soon. Integration architectures need to handle both.
One more layer to plan for: clinical terminologies. SNOMED CT, LOINC, and ICD-10 matter for any platform that ingests or displays clinical data alongside benefits data. Without shared terminology standards, the same clinical concept means different things in different systems.
Normalize Data Across Disparate Source Systems
The normalization problem becomes concrete fast: connect to 10 different HRIS platforms, and you'll get employee and benefits data in 10 different schemas, field names, and formats. Without a canonical data model, every downstream consumer writes custom parsing logic. Maintenance costs multiply with every new system added.
The solution is a canonical data model — a standardized internal schema that all source system data is mapped to before it reaches downstream consumers. This model should reflect actual domain objects:
- Employees and dependents
- Benefit elections and coverage periods
- Qualifying life events
- Contribution amounts and effective dates
For teams building HR Tech or Benefits Tech products that need connections across many HRIS, payroll, and carrier systems simultaneously, this mapping layer takes months to build and carries ongoing overhead as source systems evolve.
Bindbee, for instance, maintains normalized data models across 60+ systems with benefits-specific entities — Employee Benefits, Employer Benefits, and Dependent Benefits as distinct models — covering plan name, coverage tier, contribution amounts, effective dates, and dependent relationship mapping in a consistent schema regardless of source system.
Handle Legacy Systems with Purpose-Built Adapters
Legacy system connectivity requires a different approach than REST API integration. The SFTP-to-API Bridge pattern addresses this directly:
- Middleware ingests structured files (CSV, XML, fixed-width formats) from legacy SFTP endpoints
- Files are parsed, validated, and normalized into a standardized schema
- The normalized data is exposed through the same modern REST API endpoints as direct integrations
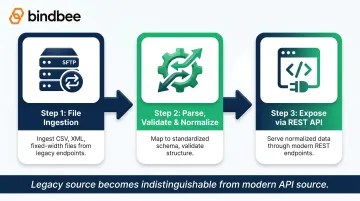
The result: downstream consumers can't distinguish between data sourced from SFTP file drops and data sourced from REST APIs. Legacy system data becomes consumable by modern applications without requiring the source system to change.
Bindbee's SFTP-to-API Bridge follows this pattern, merging SFTP-sourced and API-sourced data into a single coherent stream. This is especially relevant for carrier integrations, where SFTP remains the primary delivery mechanism.
Integration Architecture and Scalability Best Practices
Design for Scalability and Resilience from Day One
Healthcare and benefits integrations face load patterns that most B2B SaaS doesn't — open enrollment windows, new employer onboarding waves, and life event spikes can generate traffic 10x normal volume in compressed timeframes. Architecture needs to account for this upfront, not as a retrofit:
- Horizontal scaling with stateless API workers
- Caching layers for frequently-queried reference data (plan details, benefit classes)
- Load balancing across integration processing nodes
Idempotent API design is essential for healthcare workflows. Network failures, timeouts, and system downtime mean retries are inevitable — and endpoints that aren't idempotent create duplicate enrollment records, double-processed deductions, and data integrity issues that are painful to unwind.
Every write endpoint should produce the same result when called multiple times with identical input.
Implement Robust Error Handling and Retry Logic
Classify errors by type and handle them accordingly:
| Error Type | Examples | Handling |
|---|---|---|
| Transient | Network timeout, rate limit, temporary unavailability | Exponential backoff retry with jitter |
| Permanent | Invalid data, auth failure, schema violation | Fail fast, log with full context, alert |
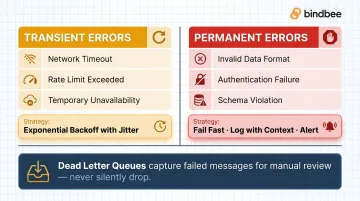
For asynchronous integrations, dead letter queues (or failed event logs) are essential. Messages that can't be processed after retries should be captured for manual review — not silently dropped. In benefits enrollment and eligibility workflows, a silently dropped message has direct consequences for employee coverage. AWS SQS, Google Cloud Pub/Sub, and equivalent services all provide native dead letter queue support.
Use Webhooks for Real-Time Event-Driven Workflows
Polling wastes resources and introduces latency. Webhooks push events the moment they occur, enabling immediate responses to qualifying life events: new hires, terminations, dependent additions, hours reductions, benefits election changes.
Webhook security requirements in the healthcare/benefits context:
- Validate HMAC-SHA256 signatures on every incoming payload — don't process webhooks that fail signature verification
- HTTPS only — no plaintext webhook delivery
- Implement idempotency to handle duplicate deliveries gracefully
- Log all received events for audit purposes
Bindbee fires webhooks for employee lifecycle events (new hires, terminations, status changes) and benefits-related events (dependent changes, qualifying life events, hours reductions), delivering structured event data that downstream systems can act on immediately rather than waiting for the next scheduled sync.
Choose Between Point-to-Point and Unified API Approaches Strategically
Point-to-point integration — building a direct connection to each carrier, HRIS, or benefits system individually — seems manageable for the first few connections. The complexity grows faster than it appears:
- Each new system adds its own authentication method, versioning schedule, and schema quirks
- Version changes in one system require changes in every system that depends on it
- Maintenance burden compounds with each new connection
When a unified API approach makes more sense:
- Your product needs connections to many systems in the same category (multiple HRIS platforms, multiple carriers)
- Maintaining one vendor relationship and one API contract is operationally preferable to managing N separate contracts
- The abstraction layer handles system-specific complexity while your team focuses on product
For teams targeting 5+ integrations in the same category, a unified API is the right call. A 3-integration build at launch looks manageable; at 10 or 15 connections, the point-to-point maintenance load becomes a real engineering liability.
Monitoring, Versioning, and Maintenance Best Practices
Monitor API Health with the Right Metrics
Track these continuously, with alerts configured to fire before thresholds are breached:
- Response time (p50, p95, p99) with SLA thresholds defined per endpoint criticality
- Error rate broken down by error type and source system
- Throughput (requests per second)
- Sync lag — time since last successful incremental data update
- Payload validation failure rate — especially important for EDI and benefits data ingestion
Structured logging in JSON format enables automated parsing and dashboarding. Every API call should produce a log entry with: timestamp, request ID, source system, data type, operation, response code, and latency. Ad hoc log searching doesn't scale when managing integrations across dozens of systems.
Manage API Versions Proactively and Maintain Integration Health
Healthcare systems update on their own schedules — carrier API changes tend to align with annual plan year cycles or regulatory updates; HRIS platforms follow quarterly SaaS release cadences with deprecation windows ranging from 90 days to 12 months.
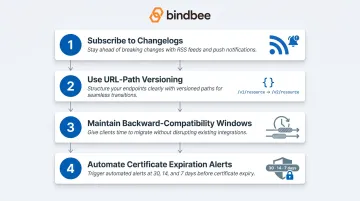
A practical change management process:
- Subscribe to vendor changelogs for every system in your integration surface
- Use URL-path versioning (/v1/resource, /v2/resource) for your own endpoints — explicit and easy to route
- Maintain backward-compatibility windows when introducing breaking changes — don't force immediate migration
- Set automated certificate expiration alerts at 30, 14, and 7 days — expired certs are one of the most common causes of integration outages
Ongoing maintenance obligations include:
- Security patching of integration middleware
- Periodic re-validation of data mappings as source systems evolve
- Quarterly review of access permissions to remove stale credentials
The "zero maintenance" model that unified API providers like Bindbee offer addresses this directly — when upstream HRIS systems change their APIs, the unified layer absorbs the change internally, and the customer-facing API contract stays stable. For teams managing connections across many systems, that distinction translates directly into engineering headcount — fewer upstream surprises means fewer engineers pulled off core product work to chase integration drift.
Frequently Asked Questions
What is API integration in healthcare?
Healthcare API integration is the process of connecting different software systems — EHRs, HRIS platforms, insurance carriers, benefits administrators — through standardized interfaces that allow them to share data automatically. This enables workflows like real-time eligibility verification, benefits enrollment sync, and clinical data exchange without manual data entry or file transfers.
What are the benefits of API integration in healthcare?
Core benefits include:
- Eliminates manual data entry and associated errors
- Maintains real-time data accuracy across connected systems
- Accelerates onboarding for employers or patients
- Reduces administrative overhead
- Improves compliance through auditable, automated data flows
For benefits platforms specifically, accurate eligibility and enrollment data also reduces coverage gaps and downstream claim issues.
What are the four types of interoperability in healthcare?
HIMSS defines four levels: foundational (systems can exchange data), structural (data is formatted consistently for interpretation), semantic (shared meaning through common terminologies like SNOMED CT and LOINC), and organizational (governance, policy, and legal frameworks that enable cross-organizational data sharing). Most integration work addresses the first two levels; semantic and organizational interoperability require broader ecosystem coordination.
What is HL7 FHIR and why does it matter?
HL7 FHIR is the leading standard for healthcare data exchange, using RESTful API conventions and standardized resource types that allow clinical and administrative systems to share data without custom transformation logic. FHIR R4 adoption is now mandated for certain payer and EHR APIs under CMS rules, making it the baseline expectation for any benefits platform interfacing with major payers.
How do you ensure HIPAA compliance in healthcare API integrations?
Key requirements:
- Implement OAuth 2.0 with scoped permissions
- Encrypt data in transit (TLS 1.2+) and at rest (AES-256)
- Maintain audit logs retained for a minimum of six years
- Execute BAAs with all vendors that process PHI
- Verify integration partners hold independent certifications like SOC 2 Type II — not just self-attestation
What is the difference between point-to-point and unified API integration?
Point-to-point builds a direct connection between each pair of systems. That works fine at 2-3 connections, but each new system multiplies the maintenance load. A unified API abstracts all those connections behind a single interface, which matters for teams supporting connections across many HRIS, carrier, or benefits systems.